January 12, 2026 – Federal Oversight Report
LOVED ONES COALITION
Weekly Oversight Report
Documenting Systemic Violations Across the Federal Bureau of Prisons
January 12, 2026
This report documents systemic abuse, neglect, retaliation, and concealment occurring across the Federal Bureau of Prisons. The conduct detailed herein is not anomalous, accidental, or confined to a single institution. It reflects an agency operating with sustained disregard for human life, statutory obligations, and constitutional limits.
A 25-year-old man is dead.
Others have been sexually assaulted while restrained.
Medically vulnerable people are being denied care, confined in unsafe isolation, and left to deteriorate.
Families are being cut off from communication, misled, or left to learn of critical events through unofficial channels.
These are not failures of communication. They are failures of custody.
The Bureau of Prisons continues to describe these outcomes as “incidents,” “emergencies,” or “staffing challenges.” The record presented here proves otherwise. Lockdowns are being used as default governance. Collective punishment has replaced individualized discipline. Medical care is delayed until collapse. Retaliation follows reporting with predictable regularity. When harm occurs, narratives are adjusted, timelines shift, and accountability disappears.
This reporting period includes a disputed custodial death with evidence contradicting the official cause, allegations of sexual assault by staff acting under color of federal authority, prolonged medical neglect following violent injury, and documented retaliation against incarcerated individuals, families, and civilian advocates. In multiple cases, Loved Ones Coalition received time-stamped reports before official disclosures, establishing notice and raising serious concerns regarding record integrity and post-incident concealment.
These conditions persist after notice.
They persist across regions.
They persist regardless of security level.
That persistence is the evidence.
The Bureau is no longer operating a correctional system capable of lawful custody. It is operating a containment model that relies on deprivation, delay, and intimidation to manage volume, staffing collapse, and institutional failure. Oversight mechanisms intended to prevent abuse are ineffective or ignored. Internal reporting channels are bypassed. Families and advocates now function as the warning system.
This report is not advisory.
It is a record.
The documentation that follows establishes exposure under the Eighth Amendment, First Amendment retaliation, Due Process violations, PREA standards, ADA and Rehabilitation Act obligations, and pattern-or-practice indicators sufficient to trigger Department of Justice Civil Rights review and criminal investigation where applicable.
Facilities named herein are on notice.
Regions implicated are on record.
Continued inaction will be treated as deliberate indifference.
What follows is a facility-by-facility accounting of misconduct, harm, and supervisory failure. The Bureau will not be given the benefit of ambiguity where evidence exists.
NORTHEAST REGION
FCI Fort Dix (New Jersey)
Jarette Fabián Morales de Jesús – FCI Fort Dix (New Jersey)
1. SUMMARY OF ALLEGATIONS
Loved Ones Coalition (LOC) is documenting the custodial death of Jarette Fabián Morales de Jesús, age 25, who died while incarcerated at FCI Fort Dix. Although the Bureau of Prisons (BOP) has publicly characterized this death as an “accident” caused by compression and postural asphyxia, LOC is in possession of photographic evidence, documentary evidence, time-stamped communications, and multiple witness accounts that materially contradict that narrative.
LOC has personally reviewed photographs of Mr. Morales’ body as it was returned to his family, reviewed the official death certificate, and analyzed time-stamped reports and tips received prior to the official date of death listed by the State of New Jersey. The physical condition of the body, combined with timeline discrepancies and testimony, raises grave concerns of excessive force, assault, and post-incident narrative manipulation.
This was not a routine custodial death.
This case presents red flags consistent with a violent death in custody and subsequent institutional concealment.
2. KEY ALLEGATIONS & EVIDENCE TABLE
| Category | Allegation / Finding |
| Official Narrative | Death classified as an “accident” caused by compression and postural asphyxia |
| Physical Evidence | LOC possesses photographs showing extensive trauma inconsistent with an accidental death |
| Body Condition | Severe facial trauma, loss of an eye, head/neck/chest injuries, discolored extremities, and post-mortem facial reconstruction |
| Autopsy Authority | Autopsy performed by New Jersey Medical Examiner, not BOP |
| Scene Control | BOP controlled the scene, custody of the body prior to transfer, and information provided to the Medical Examiner |
| Timeline Discrepancy | LOC notified of death on 11/27/2025; death certificate lists 11/29/2025 |
| Time-Stamped Evidence | LOC possesses time-stamped messages and reports that pre-date the official death date |
| Witness Testimony | Multiple accounts alleging violent assault prior to death |
| Imminent Release | Mr. Morales reportedly had approximately 50 days remaining before release |
| Institutional Risk | Potential spoliation of evidence absent immediate litigation hold |
3. PHYSICAL EVIDENCE REVIEW (NON-GRAPHIC SUMMARY)
Loved Ones Coalition has reviewed photographic evidence documenting Jarette Morales’ body as received by his family. The injuries observed include, but are not limited to:
- Extensive blunt-force trauma to the face and head
- Loss of an eye
- Severe injuries to the neck and chest region
- Discoloration of hands and fingers indicating trauma or circulatory compromise
- Evidence of post-mortem facial reconstruction, indicating catastrophic facial injury prior to death
These findings are not consistent with a simple accidental postural asphyxia scenario and are consistent with severe physical violence.
Out of respect for the family, LOC has not publicly released the full photographic record, but confirms that 27 images exist, including images taken prior to facial reconstruction.
4. AUTOPSY & MEDICAL EXAMINER CONCERNS
While the autopsy was conducted by the New Jersey Medical Examiner, LOC emphasizes:
- The BOP controlled the scene
- The BOP controlled the timeline
- The BOP controlled custody of the body prior to transfer
- The BOP supplied the initial narrative to the Medical Examiner
All communications between BOP staff and the Medical Examiner are therefore material evidence and must be reviewed to determine whether the cause and manner of death were influenced by incomplete or misleading information.
The presence of an external Medical Examiner does not absolve institutional liability.
5. TIMELINE DISCREPANCY & ADVANCE NOTICE
A critical red flag in this case is the timeline mismatch:
- Loved Ones Coalition began receiving reports and tips regarding Mr. Morales’ death on November 27, 2025
- The official death certificate lists November 29, 2025 as the date of death
LOC possesses time-stamped communications documenting this discrepancy. This raises serious concerns regarding:
- Accuracy of official records
- Timing of notifications
- Potential post-incident narrative adjustment
This discrepancy requires immediate explanation.
6. LOC POSITION
Loved Ones Coalition states unequivocally:
- We have seen the body
- We have the photographs
- We have the death certificate
- We have time-stamped evidence
- We have testimony
The evidence does not support the narrative currently being presented.
This is not speculation.
This is documentation.
7. OVERSIGHT DEMANDS
Loved Ones Coalition formally demands:
- Immediate preservation of all evidence, including video, audio, medical, forensic, and communications records
- Written confirmation of DOJ Office of Inspector General referral
- Written confirmation of DOJ Civil Rights Division referral
- Disclosure of FBI involvement, including assigned investigator if applicable
- Full release of the complete autopsy file, including photographs and examiner notes
- Written explanation of the date-of-death discrepancy
- Identification of all staff involved in any interaction with Mr. Morales prior to death
Failure to act will result in public disclosure of evidence already lawfully in LOC’s possession.
8. CONCLUSION
A 25-year-old man died in federal custody.
The injuries observed are severe.
The timeline does not match.
The evidence exists.
Loved Ones Coalition will continue escalating this case until truth, transparency, and accountability are achieved.
Justice for Jarette Fabián Morales de Jesús.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
NORTHEAST REGION
FCI McKean Satellite Prison Camp — Pennsylvania
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, FCI McKean Satellite Prison Camp is experiencing systemic failures involving retaliation, improper administration of the Residential Drug Abuse Program (RDAP), lack of required clinical oversight, First Step Act noncompliance, inadequate medical care, denial of basic services, and unsafe living conditions.
Actions and omissions by staff acting under color of federal authority have resulted in RDAP delays, improper suspensions, loss of statutory benefits, and conditions that pose a serious risk to health, safety, and constitutional rights. The scope, duration, and repetition of these failures indicate institutional and regional oversight breakdowns requiring immediate escalation.













NAMED STAFF IMPLICATED
(Accountability Index)
- Christopher Barber — RDAP Drug Treatment Specialist
Alleged conduct: Improper RDAP suspensions and delays, retaliation, lack of transparency in RDAP administration and incentives - Paula Schenfield — RDAP Drug Treatment Specialist
Alleged conduct: Improper RDAP holds and suspensions, failure to issue required RDAP incentives, lack of transparency - Mr. Hill — Unit Manager
Alleged conduct: Retaliation, interference with administrative remedies, approval of improper housing decisions affecting RDAP participants - Ms. Smith — Case Manager
Alleged conduct: Failure to properly process First Step Act placement and credits - Mr. Smith — Counselor
Alleged conduct: Retaliation and interference with administrative remedy submissions - Warden Newman — Warden
Alleged conduct: Failure of institutional oversight, inadequate medical care, denial of basic services, unsafe living conditions - Assistant Warden Price — Assistant Warden
Alleged conduct: Supervisory failures, approval of improper housing, recreation, and living conditions - Northeast Regional RDAP Oversight Personnel — Titles Unknown
Alleged conduct: Failure to ensure required RDAP staffing, oversight, and compliance
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Staff Named | Policy / Law Implicated | Impact |
| 1 | Retaliation and interference with administrative remedies | Barber; Schenfield; Hill; Ms. Smith; Mr. Smith | PS 1330.18 | Chilled reporting; denial of remedies |
| 2 | Improper RDAP suspensions and delays | Barber; Schenfield | PS 5330.11; 18 U.S.C. § 3621(e) | Loss of statutory RDAP benefits |
| 3 | Lack of required RDAP clinical staffing and oversight | Warden Newman; Assistant Warden Price; Regional RDAP personnel | PS 5330.11 | Program instability; unprofessional conduct |
| 4 | Failure to process FSA placements and credits | Ms. Smith | PS 3710.01; 18 U.S.C. §§ 3624(c), 3632 | Delayed release; loss of earned time |
| 5 | Improper commingling of RDAP and non-RDAP inmates | Hill; Assistant Warden Price | PS 5330.11 | RDAP suspensions; treatment disruption |
| 6 | Inadequate medical care | Warden Newman | PS 6031.04; PS 6000.05; 18 U.S.C. § 4042 | Serious health risks |
| 7 | Extended denial of law library access | Warden Newman | PS 1315.07 | Denial of access to courts |
| 8 | Restricted access to religious services | Warden Newman; Assistant Warden Price | PS 5360.09; RFRA | Violation of religious rights |
| 9 | Compromised nutrition and food service | Warden Newman | PS 4700.07 | Nutritional deprivation |
| 10 | Unsanitary recreation and living conditions | Warden Newman; Assistant Warden Price | 18 U.S.C. § 4042; Eighth Amendment | Health and sanitation risks |
| 11 | RDAP incentive payments not issued or accounted for | Barber; Schenfield | PS 5330.11 | Financial and program integrity concerns |
EXPANDED ALLEGATION DETAIL
Allegation 1: Retaliation and Interference with Administrative Remedies
Staff Named: Christopher Barber; Paula Schenfield; Mr. Hill; Ms. Smith; Mr. Smith
Based on corroborated reporting reviewed by Loved Ones Coalition, individuals attempting to utilize the Administrative Remedy Program report repeated obstruction, including refusal to process BP-8, BP-9, and BP-10 submissions, destruction or disappearance of remedy paperwork, and intimidation following complaints. This conduct appears designed to suppress reporting and shield staff misconduct from review.
These actions undermine the integrity of the Administrative Remedy Program and are inconsistent with BOP Program Statement 1330.18, raising serious concerns regarding retaliation and denial of protected administrative rights.
Allegation 2: Improper RDAP Suspensions and Program Delays
Staff Named: Christopher Barber; Paula Schenfield
Based on corroborated reporting reviewed by Loved Ones Coalition, RDAP participants report unexplained program holds and suspensions without written notice or documented clinical justification. These actions have directly impacted completion timelines, graduation dates, and eligibility for early-release benefits.
This pattern reflects noncompliance with BOP Program Statement 5330.11 and raises concerns regarding arbitrary program administration and deprivation of congressionally authorized incentives.
Allegation 3: Lack of Required Clinical Staffing and Oversight
Staff Named: Warden Newman; Assistant Warden Price; Northeast Regional RDAP Oversight Personnel
Based on corroborated reporting reviewed by Loved Ones Coalition, RDAP at the satellite camp operates without required on-site clinical leadership, including a Chief Psychologist, Program Coordinator, or Psychology Technician. The absence of consistent clinical oversight has resulted in inconsistent treatment delivery and unclear program decisions.
These deficiencies indicate failures at both the institutional and regional levels and undermine RDAP integrity.
Allegation 4: Failure to Properly Process First Step Act Placements and Credits
Staff Named: Ms. Smith
Based on corroborated reporting reviewed by Loved Ones Coalition, eligible RDAP participants report delays and failures in consideration of First Step Act conditional placements, particularly during Phase I participation.
These failures are inconsistent with PS 3710.01 and 18 U.S.C. §§ 3621(e), 3624(c), and 3632, resulting in delayed release and loss of earned statutory benefits.
Allegation 5: Improper Commingling of RDAP and Non-RDAP Inmates
Staff Named: Mr. Hill; Assistant Warden Price
Based on corroborated reporting reviewed by Loved Ones Coalition, non-RDAP inmates were housed with RDAP participants, resulting in program suspensions attributed to Modified Therapeutic Community violations and disruption of treatment.
Such decisions foreseeably jeopardize program integrity and conflict with RDAP operational requirements.
Allegation 6: Inadequate Medical Care
Staff Named: Warden Newman
Based on corroborated reporting reviewed by Loved Ones Coalition, medical services are primarily provided by physician assistants and intermittent nursing staff, with no licensed physician reportedly present at the camp for over fifteen months.
This prolonged absence of physician-level care raises serious concerns under PS 6031.04 and PS 6000.05 regarding access to adequate medical treatment.
Allegation 7: Extended Denial of Law Library Access
Staff Named: Warden Newman
Based on corroborated reporting reviewed by Loved Ones Coalition, prolonged institutional restrictions resulted in the law library being locked for weeks or months without alternative access.
This practice raises constitutional concerns regarding access to courts and is inconsistent with PS 1315.07.
Allegation 8: Restricted Access to Religious Services
Staff Named: Warden Newman; Assistant Warden Price
Based on corroborated reporting reviewed by Loved Ones Coalition, religious services were not consistently accessible to individuals of various faiths, with prolonged restrictions limiting religious practice.
These conditions raise concerns under PS 5360.09 and the Religious Freedom Restoration Act.
Allegation 9: Compromised Nutrition and Food Service
Staff Named: Warden Newman
Based on corroborated reporting reviewed by Loved Ones Coalition, the national menu was not consistently followed, utensils were not reliably provided, and extended periods of unit restriction resulted in cereal and bologna bag lunches with no hot meals.
Additional reporting describes meals served cold after prolonged delays during lockdowns, raising concerns under PS 4700.07.
Allegation 10: Unsanitary Recreation and Living Conditions
Staff Named: Warden Newman; Assistant Warden Price
Based on corroborated reporting reviewed by Loved Ones Coalition, a warehouse was converted into recreation space lacking bathrooms, running water, ventilation, and adequate custodial maintenance, creating ongoing sanitation and health concerns.
Allegation 11: RDAP Incentive Payments and Transparency
Staff Named: Christopher Barber; Paula Schenfield
Based on corroborated reporting reviewed by Loved Ones Coalition, RDAP participants report required phase-based incentive payments, including standard $40 payments, are not consistently issued, with no clear accounting or explanation.
This raises concerns regarding RDAP financial integrity and compliance with PS 5330.11.
CONDITIONS & DIRECT TESTIMONY
“The water coming out of the faucet and the toilet is brown and stinks. Since Monday we have had to drink, shower, and use the toilet with this water. No bottled water has been provided and no memo issued. We are melting ice for water.”
— Reporting source
“In our unit, they cut the heat every weekend. Last night it was 19 degrees. We are all getting sick.”
— Reporting source
“On lockdowns, hot meals are pushed on carts through the snow. By the time they reach us, the food is cold and then sits another 40 to 50 minutes until count clears.”
— Reporting source,
PATTERN OR PRACTICE FINDINGS
- RDAP staff are repeatedly named in reports involving retaliation, unexplained suspensions, and incentive irregularities.
- Institutional leadership has failed to correct prolonged deficiencies in medical care, food service, heating, sanitation, and access to services.
- Oversight failures persist over extended timeframes, indicating systemic misconduct rather than isolated incidents.
OVERSIGHT DEMANDS
- Immediate referral of FCI McKean Satellite Prison Camp to the DOJ Office of Inspector General
- Immediate removal of named staff from direct inmate contact pending investigation
- Preservation of all records involving named staff
- Independent review of RDAP administration, medical care, food service, and environmental conditions
- Congressional notification and inquiry
- Written assurances of non-retaliation
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
NORTHEAST REGION
FCI Schuylkill — Pennsylvania
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, FCI Schuylkill demonstrates chronic program deprivation, obstruction of rehabilitative access, censorship of educational materials, retaliation through administrative interference, and failure to accommodate documented treatment needs under the First Step Act (FSA).
For more than six years, incarcerated individuals — including long-term and life-sentenced individuals — report the absence of meaningful programming, arbitrary censorship of books and educational resources, and repeated obstruction of grievance processes. During COVID-19 lockdowns, the facility allegedly banned family-sent books, restricted educational access, and imposed exploitative purchasing practices through staff-controlled ordering channels.
Further reporting documents improper transfer decisions that interrupted active trauma treatment, ignored FSA-assessed treatment needs, and returned individuals to a facility lacking required programs. These actions reflect institutional indifference to rehabilitation, misuse of discretion in transfers, and systemic failure to support reentry, education, and mental health treatment — even where no security justification exists.
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Policy / Law Implicated | Impact |
| 1 | Absence of meaningful programming | 18 U.S.C. § 4042; FSA | Institutional stagnation |
| 2 | Censorship of books and educational materials | First Amendment; PS 5266.11 | Intellectual deprivation |
| 3 | Exploitative book-ordering practices | PS 4500.12; ethics standards | Financial abuse |
| 4 | Interference with administrative remedies | PS 1330.18 | Denial of redress |
| 5 | COVID-era excessive lockdowns without enrichment | Eighth Amendment | Psychological harm |
| 6 | Improper transfer interrupting trauma treatment | FSA; PS 5324.12 | Clinical harm |
| 7 | Failure to provide required Resolve programming | FSA Needs Assessment | Treatment denial |
| 8 | Arbitrary return transfer without justification | Due Process | Program exclusion |
| 9 | Discriminatory exclusion of lifers from programs | Equal Protection principles | Systemic inequity |
| 10 | Chronic idleness and institutional neglect | 18 U.S.C. § 4042(a)(2) | Long-term harm |
EXPANDED ALLEGATION DETAIL
Allegation 1: Chronic Absence of Meaningful Programming
For a period exceeding six years, FCI Schuylkill reportedly offered no substantive rehabilitative or vocational programming beyond generic, repetitive courses such as basic parenting or anger management — programs many individuals had already completed multiple times at other facilities.
The absence of skill-building, certification, or workforce-aligned programming renders the facility functionally custodial rather than rehabilitative.
Allegation 2: Censorship and Restriction of Educational Materials
During COVID-19 lockdowns, incarcerated individuals report that:
- The library contained only outdated fiction
- Families were banned from ordering books through Amazon or publishers
- Requests for books required staff approval
- Approved books were ordered by staff at a 30% markup
This practice restricted intellectual access, imposed financial exploitation, and chilled educational self-improvement.
Allegation 3: Administrative Remedy Interference
Multiple grievances challenging book censorship reportedly disappeared upon reaching the Regional Office. Relief was only obtained after external media and executive-level escalation, suggesting internal suppression rather than lawful resolution.
Allegation 4: Excessive Lockdowns Without Educational Mitigation
During COVID-19, individuals were confined up to 23 hours per day without books, programming, or enrichment, creating extreme psychological deprivation inconsistent with humane confinement standards.
Allegation 5: Improper Transfer Interrupting Trauma Treatment
An incarcerated individual was transferred out of Otisville — where they were actively enrolled in Resolve / Seeking Safety trauma treatment, mandated by their FSA Needs Assessment — and returned to FCI Schuylkill, a facility that does not offer the required program.
Even facility psychologists reportedly acknowledged the transfer made no clinical sense.
Allegation 6: Failure to Implement First Step Act Treatment Needs
Despite documented eligibility and placement on a waiting list for trauma treatment, the individual was housed at a facility incapable of meeting their assessed needs, constituting functional denial of treatment under the First Step Act.
Allegation 7: Discriminatory Program Access for Lifers
Reporting highlights systemic exclusion of individuals serving life sentences from programs, despite their demonstrated commitment to education, authorship, certification, and instruction of others.
This creates a paradox where individuals who repeatedly recidivate access programs more readily than those committed to long-term rehabilitation.
PATTERN OR PRACTICE FINDINGS
• Chronic absence of rehabilitative programming
• Educational censorship used as control
• Grievance interference at regional level
• Transfers used without clinical or rehabilitative justification
• Systematic exclusion of lifers from meaningful programs
• Institutional tolerance of stagnation
These findings establish systemic neglect, not isolated administrative error.
OVERSIGHT DEMANDS
Loved Ones Coalition formally demands:
• Independent review of FCI Schuylkill’s program offerings
• Audit of educational material censorship and pricing practices
• Review of all transfers interrupting active treatment
• Enforcement of First Step Act treatment placement obligations
• Preservation of grievance records and regional correspondence
• Congressional notification regarding long-term program deprivation
• DOJ Office of Inspector General investigation
SOURCE PROTECTION STATEMENT
Loved Ones Coalition does not disclose the identity or classification of reporting sources. Information contained in this report is derived from corroborated testimony, documentation, and records reviewed by the organization. Names of staff are included when confirmed, as public servants acting under color of federal authority.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
NORTHEAST REGION
USP Canaan — Pennsylvania
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, USP Canaan is the site of prolonged lockdowns, retaliatory use of restrictive housing, interference with administrative remedies, obstruction of legal and personal mail, unsafe living conditions, and chronic food deprivation. These conditions have resulted in extended confinement, loss of privileges, denial of access to courts, and persistent fear for personal safety, indicating systemic misconduct and oversight failure.
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Policy / Law Implicated | Impact |
| 1 | Prolonged lockdowns lasting weeks to months | 18 U.S.C. § 4042 | Extreme confinement; safety risk |
| 2 | Retaliatory placement in SHU | First Amendment; Due Process | Punishment for protected activity |
| 3 | False or unsupported disciplinary charges | Due Process | Loss of privileges |
| 4 | Retaliation for filing administrative remedies | PS 1330.18 | Chilled reporting |
| 5 | Interference with legal and personal mail | PS 5265.14; Access to courts | Legal prejudice |
| 6 | Unsafe living conditions and fear for safety | 18 U.S.C. § 4042 | Psychological harm |
| 7 | Inadequate food quality and portion sizes | PS 4700.07 | Nutritional deprivation |
EXPANDED ALLEGATION DETAIL
Allegation 1: Prolonged Lockdowns
Based on corroborated reporting reviewed by Loved Ones Coalition, individuals at USP Canaan report being confined to extended lockdowns lasting nearly two months, from approximately September 2025 through December 2025. During this period, movement outside the cell reportedly occurred only for showers three times per week, while restrained in handcuffs.
These lockdowns appear excessive in duration and scope, raising serious concerns regarding the routine use of restrictive confinement as a management practice rather than a temporary response to specific security needs.
Allegation 2: Retaliatory Use of SHU
Based on corroborated reporting reviewed by Loved Ones Coalition, individuals report being placed in the Special Housing Unit for minor or unsupported reasons, including in direct response to exercising protected rights. Reports indicate SHU placement following the filing of administrative remedies.
The use of restrictive housing in this manner raises serious concerns regarding retaliation and abuse of disciplinary authority.
Allegation 3: False or Unsupported Disciplinary Charges
Based on corroborated reporting reviewed by Loved Ones Coalition, individuals report being issued disciplinary charges for “threatening staff” following protected activity. After successfully challenging such charges, additional disciplinary actions were reportedly imposed, resulting in loss of all privileges.
This pattern suggests the use of disciplinary processes to punish rather than correct conduct, undermining due process protections.
Allegation 4: Retaliation for Filing Administrative Remedies
Based on corroborated reporting reviewed by Loved Ones Coalition, the filing of BP-8 and BP-9 administrative remedies has reportedly resulted in disciplinary action, SHU placement, and restriction of privileges.
Such conduct is inconsistent with BOP Program Statement 1330.18 and reflects retaliation for protected grievance activity.
Allegation 5: Interference with Legal and Personal Mail
Based on corroborated reporting reviewed by Loved Ones Coalition, outgoing mail to family members and the courts has reportedly not been delivered for extended periods. Reports include legal correspondence sent to the courts remaining undelivered for over a month.
Interference with legal mail raises serious constitutional concerns regarding access to courts and due process.
Allegation 6: Unsafe Living Conditions and Fear for Personal Safety
Based on corroborated reporting reviewed by Loved Ones Coalition, individuals report feeling unsafe for the duration of their confinement at USP Canaan and fearing for their lives more often than not.
The persistence of these conditions indicates failure by institutional leadership to ensure safe and humane confinement.
Allegation 7: Inadequate Food Quality and Portions
Based on corroborated reporting reviewed by Loved Ones Coalition, food at USP Canaan is described as consistently inadequate in both quality and portion size. Individuals report small portions and food that is routinely unpalatable.
These conditions raise concerns under BOP food service standards and compound already restrictive conditions.
CONDITIONS & DIRECT TESTIMONY
“This place is horrible. The food is disgusting and the portions are small. The lockdowns are bad. I was locked down for almost two months from September 2025 until December 2025, only coming out for a shower three times a week in handcuffs. I felt unsafe the whole time and feared for my life more times than not.”
— Reporting source
“I’ve been in the SHU. They wrote me up for exercising my right to file administrative remedies. The shot was for ‘threatening staff,’ but I beat it. Then they found me guilty of another shot and took all my privileges.”
— Reporting source
“They are playing with incoming and outgoing mail. I wrote my mother over a month ago while I was in the SHU and she still hasn’t received it. The same thing happened with mail I sent to the courts.”
— Reporting source
PATTERN OR PRACTICE FINDINGS
- Prolonged lockdowns are used for extended periods without individualized justification.
- SHU placement and disciplinary charges are repeatedly associated with protected activity.
- Mail interference affects both legal and personal correspondence.
- Food deprivation and unsafe conditions persist without corrective action.
These findings indicate systemic misconduct rather than isolated incidents.
OVERSIGHT DEMANDS
- Immediate referral of USP Canaan to the DOJ Office of Inspector General
- Preservation of all records related to lockdowns, SHU placement, disciplinary actions, mail handling, and food service
- Independent review of restrictive housing practices and retaliation allegations
- Congressional notification and inquiry
- Written assurances of non-retaliation
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
MID-ATLANTIC REGION
USP Lee — Virginia
SUMMARY OF ALLEGATIONS
Based on direct documentation, contemporaneous evidence, and corroborating reports reviewed by Loved Ones Coalition, USP Lee is implicated in serious professional misconduct involving a correctional officer engaging in public harassment, degrading and sexist language, boundary violations, and implied abuse of institutional authority.
The conduct documented in this section was directed at myself, Christine Amador, Founder of Loved Ones Coalition, and Aaron Peila, a formerly incarcerated individual and current Loved Ones Coalition Board of Directors member. I am submitting this report both as the reporting party and an impacted civilian advocate, with full documentation preserved.
The documented communications include repeated public and private harassment, prison-specific threats and language, false claims of access to organizational information, and references to future incarceration and institutional “treatment.” These communications are substantiated by screenshots, timestamps, and corroborating reports.
Despite internal reporting to Bureau of Prisons channels and the subsequent placement of the involved staff member on paid administrative leave, documented contact and public commentary continued, raising serious concerns regarding command oversight, enforcement failures, and tolerance of conduct that undermines public trust, professional standards, and institutional integrity.








NAMED STAFF IMPLICATED
(Accountability Index)
- John Fortner — Correctional Officer, USP Lee
Alleged conduct:
Public harassment of Christine Amador and Aaron Peila; sexist and degrading language; use of prison-specific threats and intimidation; references to incarceration status and future confinement; boundary violations; false claims of access to Loved Ones Coalition information; continued contact after internal reporting and placement on administrative leave. - Alleged conduct:
Failure to enforce immediate no-contact restrictions; reliance on paid administrative leave without safeguards; inadequate corrective controls after notice; tolerance of conduct creating institutional risk.
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Staff Named | Policy / Law Implicated | Impact |
| 1 | Public harassment of civilian advocate | Fortner | PS 3420.11 | Professional misconduct |
| 2 | Harassment of formerly incarcerated Board member | Fortner | First Amendment | Chilling effect |
| 3 | Use of prison language implying control or punishment | Fortner | Eighth Amendment principles | Intimidation |
| 4 | Boundary violations and off-platform contact | Fortner | BOP Code of Conduct | Safety risk |
| 5 | False claims of access to advocacy organization | Fortner | Federal ethics standards | Misrepresentation |
| 6 | Continued contact after reporting | Fortner | PS 1330.18 | Retaliation concern |
| 7 | Paid administrative leave without no-contact enforcement | USP Lee leadership | Management control failure | Ongoing harm |
| 8 | Command awareness without resolution | USP Lee leadership | Supervisory liability | Oversight breakdown |
EXPANDED ALLEGATION DETAIL
Allegation 1: Harassment of Christine Amador (Civilian Advocate)
Staff Named: John Fortner
Based on corroborated reporting reviewed by Loved Ones Coalition, John Fortner directed repeated public and private communications toward Christine Amador, Founder of Loved Ones Coalition, containing degrading, sexist, and disparaging language. Statements included false assumptions about her employment, sexualized insults, and references implying familiarity with her personal life and future prison visits.
Such conduct represents a clear professional boundary violation and creates the appearance of leveraging institutional authority against a civilian advocate.
Allegation 2: Harassment of Aaron Peila (Formerly Incarcerated Board Member)
Staff Named: John Fortner
Fortner repeatedly targeted Aaron Peila, formerly incarcerated and now a Loved Ones Coalition Board of Directors member, using prison-specific slurs, references to yard status, strip-search language, and threats of future incarceration. These statements directly invoke carceral power dynamics and are incompatible with ethical standards governing correctional officers.
Allegation 3: Implied Threats and Institutional Intimidation
Staff Named: John Fortner
The communications included language such as “stand for count,” “bend and spread,” references to “treatment,” and statements about future incarceration. Regardless of claimed intent, such language cannot be divorced from the authority of a federal correctional officer and reasonably conveys intimidation.
Allegation 4: Continued Contact After Reporting and Administrative Leave
Staff Named: John Fortner
Following formal reporting to Bureau of Prisons channels, Fortner was reportedly placed on paid administrative leave. Despite this, reporting indicates continued contact and public commentary directed at both Christine Amador and Aaron Peila.
The absence of enforced no-contact restrictions reflects a failure of supervisory control and risk mitigation.
Allegation 5: Institutional Handling and Command Oversight Failures
Staff Named: USP Lee Leadership
Reporting from current and former staff indicates awareness of the situation within the institution. The reliance on paid administrative leave without immediate boundary enforcement or corrective safeguards raises concerns that misconduct was managed administratively rather than addressed substantively.
CONDITIONS & DIRECT QUOTATIONS
(Public Statements, Verbatim)
Selected public comments authored by John Fortner include:
- “Stay in your lane… wait until you get locked back up again.”
- “Stand for count and bend and spread.”
- “I’ll make sure y’all are treated properly.”
These statements are documented in screenshots reviewed by Loved Ones Coalition and are cited to establish tone, content, and professional impropriety.
PATTERN OR PRACTICE FINDINGS
- Correctional authority was invoked outside official duties.
- Sexist and degrading language was used toward a civilian advocate.
- Former incarceration status was weaponized against a Board member.
- Paid administrative leave did not halt misconduct.
- Command-level controls failed to prevent continued harassment.
These findings reflect systemic risk, not isolated online conflict.
OVERSIGHT DEMANDS
Loved Ones Coalition formally demands:
- Immediate DOJ Office of Inspector General review of the conduct
- Preservation of all digital communications involving John Fortner
- Enforcement of strict no-contact orders
- Review of USP Lee supervisory handling of staff misconduct
- Mandatory ethics and boundary training for involved personnel
- Written assurances of non-retaliation toward advocates and Board members
SOURCE & POSITION STATEMENT
Christine Amador and Aaron Peila are named by consent.
Christine Amador is the Founder of Loved Ones Coalition, the reporting party, and an impacted civilian advocate in this matter.
Aaron Peila is a formerly incarcerated individual and a current Loved Ones Coalition Board of Directors member.
Both are acting in their official capacities with Loved Ones Coalition, a national prison oversight and advocacy organization. This report is submitted to document professional misconduct, preserve accountability, prevent escalation, and protect incarcerated individuals, advocates, and families from downstream harm.
MID-ATLANTIC REGION
SFF Hazelton — West Virginia
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, SFF Hazelton is the site of severe allegations involving excessive use of force, failure to decontaminate following chemical agent exposure, misuse of four-point restraints, sexual assault, sexual abuse, and institutional failure to protect individuals confined in restrictive housing.
The conduct described involves staff acting under color of federal authority and includes allegations of criminal sexual misconduct, abuse of power, and gross violations of Bureau of Prisons policy, federal law, and constitutional protections. The seriousness and nature of these allegations require immediate escalation, external investigation, and protective intervention.
NAMED STAFF IMPLICATED
(Accountability Index)
- It Chastnik — Correctional Officer
Alleged conduct: Excessive use of chemical agents (MK-4), failure to decontaminate after chemical exposure, improper use of four-point restraints, sexual assault and sexual abuse of a restrained individual in SHU, repeated predatory conduct
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Staff Named | Policy / Law Implicated | Impact |
| 1 | Excessive use of chemical agents (MK-4) | It Chastnik | Use-of-Force Standards; 18 U.S.C. § 4042 | Physical injury; chemical burns |
| 2 | Failure to decontaminate after chemical exposure | It Chastnik | BOP Use-of-Force Policy | Prolonged physical harm |
| 3 | Improper use of four-point restraints | It Chastnik | Use-of-Restraints Policy | Severe physical and psychological trauma |
| 4 | Sexual assault and sexual abuse in SHU | It Chastnik | PREA; Eighth Amendment; federal criminal law | Sexual violence |
| 5 | Sexual exploitation of a restrained individual | It Chastnik | PREA; Due Process | Abuse of authority |
| 6 | Retaliatory confinement and isolation | It Chastnik | Due Process | Continued victimization |
| 7 | Failure of institutional protection | Institutional leadership | 18 U.S.C. § 4042 | Ongoing risk to others |
EXPANDED ALLEGATION DETAIL
Allegation 1: Excessive Use of Chemical Agents
Staff Named: It Chastnik
Based on corroborated reporting reviewed by Loved Ones Coalition, an individual confined at SFF Hazelton reports being subjected to MK-4 chemical spray while housed in the Special Housing Unit despite no reported conduct justifying such force. The exposure caused severe burning and physical distress.
The reported use of chemical agents appears excessive and unjustified, raising serious concerns regarding compliance with BOP use-of-force standards and duty-of-care obligations.
Allegation 2: Failure to Decontaminate After Chemical Exposure
Staff Named: It Chastnik
Based on corroborated reporting reviewed by Loved Ones Coalition, following MK-4 exposure, the individual was not decontaminated. The failure to provide decontamination prolonged physical suffering and increased risk of injury.
Denial of decontamination after chemical exposure constitutes a serious violation of use-of-force protocols and basic medical standards.
Allegation 3: Improper Use of Four-Point Restraints
Staff Named: It Chastnik
Based on corroborated reporting reviewed by Loved Ones Coalition, the individual was placed in four-point restraints for approximately six hours following the chemical agent incident. The restraints were applied despite the absence of conduct warranting such extreme measures.
The prolonged use of restraints under these conditions raises concerns regarding punitive restraint practices and excessive force.
Allegation 4: Sexual Assault and Sexual Abuse in SHU
Staff Named: It Chastnik
Based on corroborated reporting reviewed by Loved Ones Coalition, while confined in SHU cell 116, the individual reports repeated sexual abuse and sexual assault by the named officer. The individual reports being left in paper clothing positioned in a manner that exposed intimate body parts, after which the officer entered the cell and sexually assaulted the individual, including digital penetration.
These allegations constitute serious violations of the Prison Rape Elimination Act, the Eighth Amendment, and federal criminal law.
Allegation 5: Sexual Exploitation of a Restrained Individual
Staff Named: It Chastnik
Based on corroborated reporting reviewed by Loved Ones Coalition, the alleged sexual abuse occurred while the individual was restrained and fully under staff control, rendering the individual incapable of consent.
Sexual contact under these conditions constitutes sexual exploitation and abuse of authority and represents one of the most serious forms of staff misconduct.
Allegation 6: Retaliatory Confinement and Isolation
Staff Named: It Chastnik
Based on corroborated reporting reviewed by Loved Ones Coalition, the individual reports continued confinement and isolation following the incident, compounding trauma and further restricting access to assistance or reporting mechanisms.
Such conduct raises concerns regarding retaliation and deliberate isolation of a victim following abuse.
Allegation 7: Failure of Institutional Protection
Staff Named: Institutional leadership
Based on corroborated reporting reviewed by Loved Ones Coalition, the presence of multiple reports involving the same officer raises serious concerns regarding institutional failure to intervene, supervise, or protect individuals from known risks.
The existence of multiple victims suggests systemic breakdown rather than isolated misconduct.
PATTERN OR PRACTICE FINDINGS
- The same officer is implicated in multiple reports involving sexual abuse and excessive force.
- Chemical agents, restraints, and isolation appear to be used as tools of control rather than last-resort safety measures.
- Institutional safeguards failed to prevent repeated abuse or remove the officer from contact with vulnerable individuals.
- The conditions described indicate systemic failures in supervision, reporting, and protection.
OVERSIGHT DEMANDS
- Immediate referral of SFF Hazelton to the DOJ Office of Inspector General
- Immediate removal of the named officer from all inmate contact pending investigation
- Preservation of all records related to use of force, restraints, SHU placements, and PREA complaints
- Independent PREA investigation by external authorities
- Congressional notification and inquiry
- Immediate protective measures for any individual cooperating with investigation
- Written assurances of non-retaliation
SOURCE PROTECTION STATEMENT
Loved Ones Coalition does not disclose the identity or classification of reporting sources. Information contained in this report is derived from corroborated documentation, testimony, and records reviewed by the organization. This intentional source protection is necessary due to documented patterns of retaliation within the Federal Bureau of Prisons. Staff names are included deliberately and in full, as public servants acting under color of federal authority.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
Southeast Region—FPC Talladega
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, FPC Talladega is experiencing systemic failures involving unsafe and degrading housing conditions, fraud, waste and abuse of federal property, staff misconduct and disciplinary manipulation, environmental health hazards (including widespread mold and poor air quality), and retaliatory deprivation of basic necessities following protected reporting.
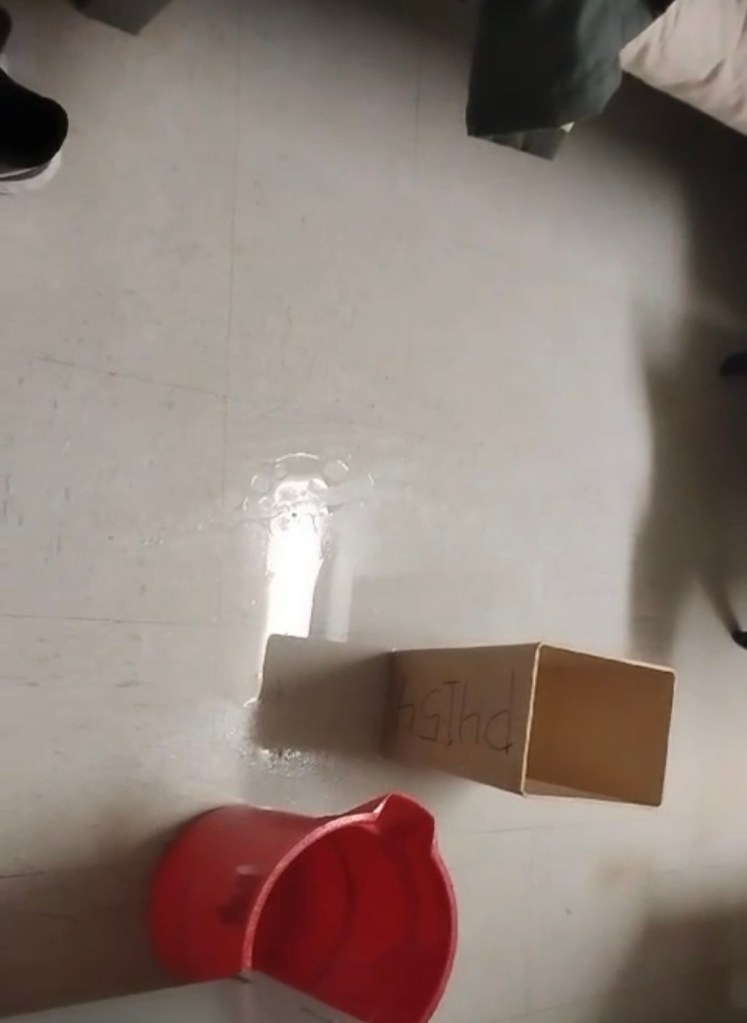
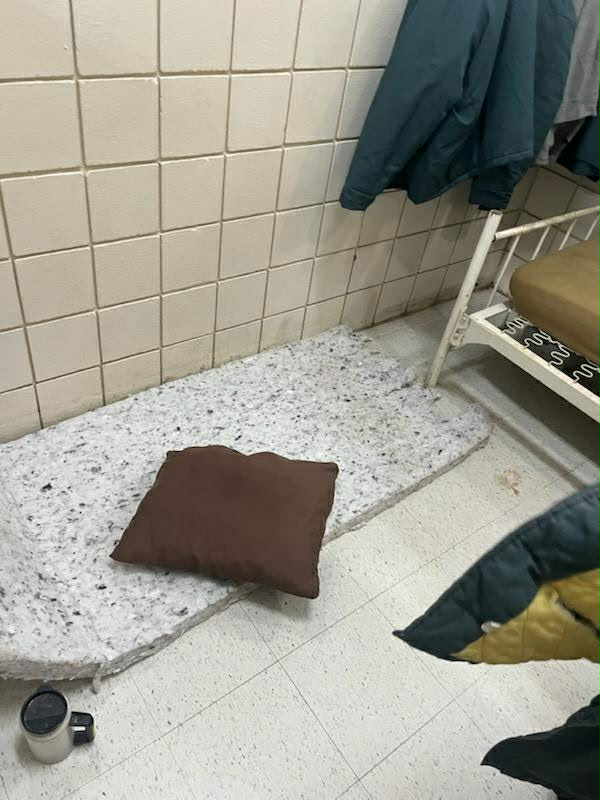
On or about January 6, 2026, newly transferred individuals were placed into active housing units without beds, bed frames, or rails and were forced to sleep directly on concrete floors using torn or partial mattress fragments. Subsequent reporting establishes that the facility possessed beds and/or brand-new mattresses at the time of the violation and withheld issuance until leadership visibility forced action.
The reported conduct reflects deliberate indifference and institutional prioritization of inspection optics over lawful, humane confinement. The timeline further indicates retaliation after escalation, including restriction of hygiene necessities such as toilet paper. The scope, sequence, and repetition of these failures indicate institutional oversight breakdown requiring immediate escalation and external investigation.
















NAMED STAFF IMPLICATED
(Accountability Index)
- Officer Mugo — Correctional Officer
Alleged conduct: Fabrication and manipulation of incident reports; use of vague and unverifiable reporting language; contradictory timelines; alleged contraband planting; retaliatory enforcement practices; repeated use as an enforcement tool during contraband incidents. - Facility Administration — FPC Talladega (Names Pending Disclosure)
Alleged conduct: Continuation of transfers despite known lack of beds; failure to provide minimum housing standards; withholding federally owned mattresses/beds; misrepresentation of compliance during inspections; tolerance of staff misconduct; retaliation through deprivation of basic necessities; failure to remediate environmental health hazards. - Senior Leadership — FPC Talladega (Warden and Executive Staff; Names Pending Disclosure)
Alleged conduct: Supervisory failures; corrective intervention only after exposure; failure to prevent retaliation; failure to implement sustained remediation; failure to involve medical and environmental health review despite known hazards.
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Staff Named | Policy / Law Implicated | Impact |
| 1 | Forced floor sleeping without beds/frames at intake (Jan 6, 2026) | Facility Administration | PS 5500.14; 18 U.S.C. § 4042; Eighth Amendment | Unsafe confinement; physical harm; degradation |
| 2 | Continuation of transfers despite known lack of housing capacity | Facility Administration | 18 U.S.C. § 4042(a)(2) | Foreseeable harm; institutional liability |
| 3 | Fraud, Waste & Abuse — mattress hoarding / inspection optics | Facility Administration | PS 1237.13; PS 1100.05; 31 U.S.C. § 3729; OMB A-123 | Misuse of federal funds; false compliance |
| 4 | Withholding federally owned mattresses/beds until exposure | Facility Administration; Senior Leadership | PS 1100.05; PS 5500.14 | Deprivation of basic necessities |
| 5 | Retaliatory restriction of toilet paper / hygiene necessities | Facility Administration | PS 1330.18; First Amendment; Eighth Amendment | Hygiene deprivation; chilled reporting |
| 6 | Staff misconduct — fabricated or unreliable incident reporting | Officer Mugo | PS 3420.11; PS 5270.09; Fifth Amendment Due Process | Arbitrary discipline; rights violations |
| 7 | Alleged contraband planting and disciplinary manipulation | Officer Mugo | PS 5270.09; Wolff v. McDonnell; Hines v. Gomez | Invalid discipline; retaliation risk |
| 8 | Widespread mold and poor ventilation/air filtration | Facility Administration | PS 1600.11; PS 4200.12; 18 U.S.C. § 4042; Eighth Amendment | Respiratory risk; chronic exposure |
| 9 | Failure to remediate environmental hazards despite awareness | Facility Administration; Senior Leadership | PS 1600.11; Farmer v. Brennan | Deliberate indifference threshold |
| 10 | Failure to involve medical/environmental health review after exposure | Senior Leadership | PS 6031.04 | Health risk unassessed; continued exposure |
EXPANDED ALLEGATION DETAIL
Allegation 1: Forced Floor Sleeping Without Beds/Frames at Intake (January 6, 2026)
Staff Named: Facility Administration
Based on corroborated reporting reviewed by Loved Ones Coalition, newly arriving individuals at FPC Talladega were assigned to active housing units without beds, bed frames, or rails and were forced to sleep directly on concrete floors using torn or partial mattress fragments. Reporting indicates staff acknowledged a “lack of bed frames and rails,” yet transfers continued under normal operations.
This conduct violates minimum housing standards and exposes individuals to injury, illness, and unsanitary confinement conditions.
Allegation 2: Continuation of Transfers Despite Known Lack of Housing Capacity
Staff Named: Facility Administration
Based on corroborated reporting reviewed by Loved Ones Coalition, the institution continued receiving transfers despite known inability to provide basic bedding/housing standards. No pause, overflow plan, or temporary humane accommodations were implemented.
This establishes foreseeable harm and institutional inaction rather than unavoidable circumstance.
Allegation 3: Fraud, Waste & Abuse — Mattress Hoarding and Inspection Optics
Staff Named: Facility Administration
Based on corroborated reporting reviewed by Loved Ones Coalition, Talladega Camp has engaged in a pattern for at least two years involving annual mattress purchases using federal funds, storage of unused mattresses, and utilization of stored mattresses as display items during inspections to falsely indicate compliance.
This pattern constitutes fraud, waste, and abuse through misrepresentation of compliance and failure to deploy government-owned property for its intended purpose.
Allegation 4: Withholding Mattresses/Beds Until Exposure Forced Action
Staff Named: Facility Administration; Senior Leadership
Based on corroborated reporting reviewed by Loved Ones Coalition, following escalation and leadership visibility on or about January 6, mattresses were issued rapidly. The speed of correction indicates that mattresses and/or beds were available at the time individuals were sleeping on concrete and were withheld until exposure forced action.
This confirms institutional knowledge and optics-driven compliance rather than sustained adherence to standards.
Allegation 5: Retaliation Through Restriction of Toilet Paper and Hygiene Necessities
Staff Named: Facility Administration
Based on corroborated reporting reviewed by Loved Ones Coalition, after the incident was reported and leadership intervened, incarcerated individuals experienced restriction of toilet paper and related hygiene necessities through delayed distribution and limited issuance.
The timing and sequence strongly indicate retaliatory deprivation following protected reporting, not legitimate shortage management.
Allegation 6: Staff Misconduct — Unethical and Potentially Unlawful Conduct by Officer Mugo
Staff Named: Officer Mugo
Based on corroborated reporting reviewed by Loved Ones Coalition, Officer Mugo is routinely utilized by administration during contraband incidents and is associated with repeated use of vague and unverifiable incident-report language, lack of corroboration, contradictory timelines, and allegations of fabricated enforcement.
This pattern raises serious concerns regarding disciplinary integrity, due process violations, and retaliatory enforcement.
Allegation 7: Alleged Contraband Planting and Evidence Fabrication
Staff Named: Officer Mugo
Multiple reports reviewed by Loved Ones Coalition describe conduct consistent with contraband being placed in living areas or attributed to individuals without reliable evidentiary support. This undermines disciplinary legitimacy and raises constitutional concerns under due process standards.
Allegation 8: Mold Infestation, Poor Ventilation, and Lack of Air Filtration
Staff Named: Facility Administration
Based on corroborated reporting reviewed by Loved Ones Coalition, Talladega Camp exhibits widespread mold in showers and housing areas, contaminated vents/air pathways, and lack of adequate filtration or ventilation. Photographic documentation reviewed by LOC supports persistent environmental hazards.
Incarcerated individuals cannot remove themselves from exposure, creating ongoing health risk.
Allegation 9: Failure to Remediate Environmental Hazards Despite Awareness
Staff Named: Facility Administration; Senior Leadership
Based on corroborated reporting reviewed by Loved Ones Coalition, mold and air-quality hazards have persisted over extended timeframes, indicating administrative awareness without corrective action. Continued exposure after notice meets the deliberate indifference threshold where known risks are disregarded.
Allegation 10: Failure to Conduct Medical/Environmental Health Review After Exposure
Staff Named: Senior Leadership
Based on corroborated reporting reviewed by Loved Ones Coalition, leadership intervention focused on immediate optics corrections (issuing bedding) without documented medical screening, environmental inspection, or remediation planning despite known mold and sanitation issues. This constitutes supervisory failure under patient care and safety obligations.
CONDITIONS & DIRECT TESTIMONY
“We were forced to sleep on concrete with torn mattress pieces. After everything got reported, leadership came and beds showed up immediately.”
— Reporting source
“They restricted toilet paper right after it got reported.”
— Reporting source
“The mold is everywhere. Nothing got fixed — they just brought beds.”
— Reporting source
PATTERN OR PRACTICE FINDINGS
- Unsafe housing practices occurred despite availability of resources, suggesting deliberate deprivation rather than inability.
- Federal property appears withheld to preserve inspection optics, indicating fraud/waste exposure.
- Leadership action occurred only after exposure, confirming oversight failure.
- Retaliatory deprivation followed protected reporting, indicating a chilled reporting environment.
- Environmental hazards persist without remediation, compounding health and liability risk.
- Staff misconduct allegations continue with administrative reliance/tolerance.
These findings indicate systemic misconduct rather than isolated operational failure.
OVERSIGHT DEMANDS
- Immediate referral of FPC Talladega to the DOJ Office of Inspector General
- Preservation of all records related to: mattress procurement, inventory logs, bed assignments, intake rosters, inspection materials, and housing capacity decisions
- Independent Fraud, Waste & Abuse audit of mattress purchases, storage, and inspection representations
- Independent investigation of Officer Mugo, including review of all incident reports authored by him and associated disciplinary outcomes
- Emergency environmental inspection and mold remediation assessment by qualified professionals
- Installation/verification of ventilation and air filtration consistent with federal health standards
- Written corrective action plan with deadlines, accountability assignments, and compliance verification
- Written assurances of non-retaliation for all reporting individuals
SOURCE PROTECTION STATEMENT
Loved Ones Coalition does not disclose the identity or classification of reporting sources. Information contained in this report is derived from corroborated documentation, testimony, and records reviewed by the organization. This intentional source protection is necessary due to documented patterns of retaliation within the Federal Bureau of Prisons. Staff names are included deliberately and in full when identified, as public servants acting under color of federal authority.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
SOUTHEAST REGION
FCC Coleman (USP Coleman I) — Florida
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, FCC Coleman (USP Coleman I) is experiencing continuous lockdowns, extreme movement restrictions, prolonged delays in approved transfers, staff attrition without continuity of case management, and serious safety concerns, including reported deaths and lack of staff presence during critical incidents.
The conditions described reflect systemic operational breakdowns rather than isolated incidents. Persistent lockdowns, reduced access to recreation and social contact, failure to execute approved transfers, and apparent absence of staff oversight raise urgent concerns regarding institutional management, safety, and accountability.
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Policy / Law Implicated | Impact |
| 1 | Continuous lockdowns since February | 18 U.S.C. § 4042 | Prolonged confinement; mental health harm |
| 2 | Extreme movement restrictions and unit isolation | 18 U.S.C. § 4042 | Social isolation; reduced recreation |
| 3 | Fragmented recreation yard access | BOP recreation standards | Limited outdoor activity |
| 4 | Failure to execute approved camp transfers | PS 5100.08; FSA framework | Unlawful delay of placement |
| 5 | Case manager resignation without continuity | BOP staffing obligations | Administrative paralysis |
| 6 | Staff absence during emergencies | 18 U.S.C. § 4042 | Safety failures |
| 7 | Unexplained deaths and lack of transparency | Duty of care obligations | Risk to life; family distress |
EXPANDED ALLEGATION DETAIL
Allegation 1: Continuous Lockdowns
Based on corroborated reporting reviewed by Loved Ones Coalition, FCC Coleman (USP Coleman I) has been subject to near-constant lockdowns since February. These lockdowns are described as occurring back-to-back with minimal relief, creating an environment of prolonged confinement.
Extended lockdowns of this nature raise serious concerns regarding excessive restriction, mental health impact, and reliance on lockdowns as a routine operational practice rather than a limited response to specific security incidents.
Allegation 2: Extreme Movement Restrictions and Unit Isolation
Based on corroborated reporting reviewed by Loved Ones Coalition, only three units—H Unit, F Unit, and the worker unit (A Unit)—are operating as program units. All remaining housing units are reportedly on modified movement, with tiers alternating access on different days.
This structure prevents meaningful interaction beyond one’s own unit and results in extreme social isolation, significantly altering normal movement and program expectations.
Allegation 3: Fragmented Recreation Yard Access
Based on corroborated reporting reviewed by Loved Ones Coalition, the recreation yard has been divided into three separate sections, with two units assigned per section at any given time. Each unit is released separately, substantially reducing outdoor recreation time.
As a result, individuals report significantly diminished access to outdoor recreation and the inability to interact with anyone outside their assigned unit, compounding isolation and confinement conditions.
Allegation 4: Failure to Execute Approved Camp Transfers
Based on corroborated reporting reviewed by Loved Ones Coalition, individuals approved for camp placement have remained at their current institution for over a month without transfer. In at least one case, approval was granted, but no action was taken to effectuate the transfer.
Failure to execute approved placements undermines First Step Act implementation and results in unnecessary continued confinement at higher-security settings.
Allegation 5: Case Manager Resignation Without Continuity
Based on corroborated reporting reviewed by Loved Ones Coalition, a case manager responsible for processing transfers and placements resigned, leaving approved individuals without continuity of case management or reassignment.
This administrative breakdown has resulted in stalled placements, lack of communication, and uncertainty regarding sentence progression, reflecting broader staffing and accountability failures.
Allegation 6: Staff Absence During Emergencies
Based on corroborated reporting reviewed by Loved Ones Coalition, staff were reportedly not present or immediately available during a critical incident occurring in the early morning hours, approximately between 2:00 and 3:00 a.m.
The absence of staff presence during emergencies raises serious concerns regarding institutional readiness, supervision, and duty of care.
Allegation 7: Unexplained Deaths and Lack of Transparency
Based on corroborated reporting reviewed by Loved Ones Coalition, an individual was reportedly removed from the facility after staff believed the person had passed away during the early morning hours. Reporting indicates that deaths within the facility are perceived as frequent, with limited transparency or communication.
These reports raise urgent concerns regarding safety, medical response, and institutional accountability.
CONDITIONS & DIRECT TESTIMONY
“Since February, it has been lockdown after lockdown non-stop. There are only three program units now. The rest of the compound is on modified movement, one tier out one day and the other tier the next. The yard is split into three sections and we never see anyone outside our unit. Outside rec time has been cut way down.”
— Reporting source
“My husband was approved for the camp over a month ago, but they still haven’t transferred him. His case manager resigned and nothing is moving. This feels systematic across the BOP.”
— Reporting source
“He said a younger white male was hauled away this morning. They believe he passed around 2–3 a.m. COs were nowhere to be found. The deaths inside are unreal.”
— Reporting source
PATTERN OR PRACTICE FINDINGS
- Lockdowns are continuous and prolonged, functioning as a routine operational condition.
- Movement restrictions and yard fragmentation severely limit recreation and human contact.
- Approved transfers are not executed in a timely manner.
- Staff attrition is not accompanied by continuity planning.
- Critical incidents occur without adequate staff presence or transparency.
These findings reflect systemic operational failures rather than isolated incidents.
OVERSIGHT DEMANDS
- Immediate referral of FCC Coleman (USP Coleman I) to the DOJ Office of Inspector General
- Preservation of all records related to lockdowns, movement restrictions, staffing assignments, transfers, and critical incidents
- Independent review of First Step Act and camp-transfer implementation
- Review of staffing levels, overnight supervision, and emergency response protocols
- Congressional notification and inquiry
- Written assurances of non-retaliation for individuals cooperating with oversight
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
SOUTHEAST REGION
FCI Edgefield — South Carolina
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, FCI Edgefield is the site of a documented and escalating pattern of retaliation, abuse of authority, disciplinary manipulation, family-contact interference, and staff-confirmed misconduct involving named officers.
This entry reflects continued retaliation following formal notice, including retaliatory discipline, threats of SHU placement, manipulation of incident reports, humiliating strip searches following visitation, and interference with family contact. The conduct described has been confirmed by currently employed Bureau of Prisons staff, continued after notice to Bureau leadership and Internal Affairs, and now reflects deliberate indifference and systemic failure.
NAMED STAFF IMPLICATED
(Accountability Index)
- Officer Glass — Correctional Officer
Alleged conduct: Retaliatory discipline, verbal intimidation, threats of SHU placement, escalation and stacking of incident reports, ignoring exculpatory statements - Officer Williams — Correctional Officer
Alleged conduct: Participation in retaliatory discipline, continued staff contact after formal retaliation notice, abuse of authority - Officer Almond — Correctional Officer
Alleged conduct: Targeted and repeated strip searches following visitation, humiliating treatment inconsistent with peer handling, abuse of authority - SIS Officer Pestory — SIS Officer
Alleged conduct: Conflicting representations regarding investigation closure and housing status, contributing to prolonged SHU confinement without explanation - Facility Administration — Institutional Leadership
Alleged conduct: Failure to intervene, deliberate indifference following notice, tolerance of retaliatory conduct
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Staff Named | Policy / Law Implicated | Impact |
| 1 | Retaliatory discipline following protected family advocacy | Glass; Williams | First Amendment | Punishment for protected activity |
| 2 | Verbal threats of SHU placement as intimidation | Glass | Abuse of Authority | Chilling effect |
| 3 | Escalation and stacking of incident reports | Glass | Due Process | Increased sanctions |
| 4 | Ignoring exculpatory statements | Glass | Wolff v. McDonnell | Procedural violations |
| 5 | Continued staff contact after retaliation notice | Glass; Williams | Deliberate Indifference | Ongoing risk |
| 6 | Targeted strip searches following visitation | Almond | PREA; Fourth & Eighth Amendments | Humiliation; abuse |
| 7 | Family contact interference | Almond; Facility staff | Visitation standards | Emotional harm |
| 8 | Prolonged SHU confinement after investigation closure | Pestory; Administration | Due Process | Unlawful isolation |
| 9 | Failure of leadership intervention | Facility Administration | 18 U.S.C. § 4042(a)(2) | Systemic liability |
EXPANDED ALLEGATION DETAIL
Allegation 1: Retaliatory Discipline Following Protected Family Advocacy
Staff Named: Officer Glass; Officer Williams
Based on corroborated reporting reviewed by Loved Ones Coalition, disciplinary actions were taken against an incarcerated individual following protected family advocacy related to conditions and staff conduct at FCI Edgefield. Staff-confirmed reporting establishes that these disciplinary actions were retaliatory in nature and not supported by neutral enforcement standards.
The retaliatory conduct was known to LOC through staff communications before families were notified, demonstrating internal awareness of improper discipline and a failure to correct it.
Allegation 2: Verbal Threats of SHU Placement as Intimidation
Staff Named: Officer Glass
Based on corroborated reporting reviewed by Loved Ones Coalition, Officer Glass issued verbal threats of SHU placement, including statements asserting authority to do so “because he can,” in front of others. These threats were tied to prior advocacy and functioned as intimidation rather than legitimate discipline.
Such conduct reflects abuse of authority and retaliation, not corrective enforcement.
Allegation 3: Escalation and Stacking of Incident Reports
Staff Named: Officer Glass
During a dormitory search, contraband was discovered in a shared living space. Another individual explicitly accepted responsibility for the item. Despite this admission, Officer Glass issued disciplinary charges to both individuals and added a more severe charge only to the individual associated with prior family advocacy.
Staff later confirmed to LOC that this escalation was not justified. This conduct reflects retaliatory enforcement and manipulation of the disciplinary process.
Allegation 4: Ignoring Exculpatory Statements
Staff Named: Officer Glass
Based on corroborated reporting reviewed by Loved Ones Coalition, exculpatory statements were disregarded during disciplinary proceedings, despite clear admissions by another individual. This omission violates due-process standards articulated in Wolff v. McDonnell and undermines the legitimacy of disciplinary outcomes.
Allegation 5: Continued Staff Contact After Formal Retaliation Notice
Staff Named: Officer Glass; Officer Williams
Prior to the above actions, LOC formally placed the Bureau of Prisons on notice regarding retaliation risks at FCI Edgefield, identifying Officer Glass and Officer Williams. Despite this notice, no staff separation occurred, no interim protections were implemented, and retaliatory conduct continued and escalated.
Continuation of contact after notice constitutes deliberate indifference.
Allegation 6: Targeted Strip Searches Following Visitation
Staff Named: Officer Almond
Based on corroborated reporting reviewed by Loved Ones Coalition, Officer Almond conducted targeted strip searches following visitation that were applied to one individual while others were either patted down or not searched at all. This conduct has occurred more than once and is described as humiliating and inconsistent with peer treatment.
The strip searches occurred in the presence of family members, resulting in emotional harm and distress, including children witnessing abrupt separation. This raises serious concerns under PREA standards and constitutional protections.
Allegation 7: Family Contact Interference
Staff Named: Officer Almond; Facility Staff
Following visitation, the affected individual was delayed and prevented from exiting normally, depriving family members— including children—of final contact. Reporting indicates family members recognized the pattern based on prior incidents involving the same officer.
This conduct interferes with family contact and compounds retaliatory impact.
Allegation 8: Prolonged SHU Confinement After Investigation Closure
Staff Named: SIS Officer Pestory; Facility Administration
After Internal Affairs dismissed an investigation for lack of evidence and SIS Officer Pestory informed the family that the individual would return to the camp compound, the individual remained confined in SHU without explanation.
This unexplained continued confinement raises serious due-process concerns.
Allegation 9: Failure of Leadership Intervention
Staff Named: Facility Administration
Despite repeated notice, staff-confirmed reporting, and escalating retaliation, leadership failed to intervene, separate staff, or implement protections. This inaction has allowed continued misconduct and exposed the institution to significant constitutional and federal liability.
CONDITIONS & DIRECT TESTIMONY
“This is the second time the same officer has done it. It’s very humiliating. Everyone else was patted down or not searched at all. The officer’s name is Almond.”
— Reporting source
“Our kids were waiting to wave to him one last time and he never came out. I knew what was happening because the same officer did it before.”
— Reporting source
“ the discipline was retaliation.”
— Reporting source with direct knowledge, identity protected
PATTERN OR PRACTICE FINDINGS
- Retaliation following family advocacy is repeated and escalating
- Disciplinary authority is used as punishment, not enforcement
- Exculpatory evidence is ignored
- Strip searches are selectively and punitively applied
- Staff-confirmed misconduct continues after notice
- Leadership fails to intervene
These findings establish systemic retaliation, not isolated incidents.
OVERSIGHT DEMANDS — FCI EDGEFIELD
Loved Ones Coalition formally demands:
- Immediate preservation of all incident reports, SIS notes, disciplinary records, visitation logs, and camera footage involving Officers Glass, Williams, and Almond
- Immediate separation of Officers Glass, Williams, and Almond from enforcement authority pending review
- Independent review of retaliatory discipline and strip-search practices
- Disclosure of actions taken after prior retaliation notice
- On-site regional leadership review
- Written confirmation that retaliation will not be tolerated or concealed
Failure to act will be documented as institutional complicity.
SOURCE PROTECTION STATEMENT
Loved Ones Coalition does not disclose the identity or classification of reporting sources. Information contained in this report is derived from corroborated documentation, testimony, and records reviewed by the organization. This intentional source protection is necessary due to documented patterns of retaliation within the Federal Bureau of Prisons. Staff names are included deliberately and in full, as public servants acting under color of federal authority.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
SOUTH CENTRAL REGION
USP Pollock — Louisiana
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, USP Pollock is the site of serious failures involving inmate safety, failure to notify next of kin following a violent assault, denial and delay of medically necessary care, inhumane Special Housing Unit (SHU) conditions, obstruction of information to family members, and systemic medical neglect following traumatic injury.
The reporting describes a violent assault resulting in severe facial and orbital fractures, followed by prolonged SHU confinement under unsafe and unsanitary conditions, lack of timely and adequate medical intervention, failure to follow established injury protocols, and institutional refusal to provide transparency or accountability.
These conditions present significant risks to life, permanent disability, and constitutional rights and reflect systemic operational and medical failures rather than isolated incidents.
NAMED STAFF IMPLICATED
(Accountability Index)
Facility Administration — USP Pollock
Alleged conduct: Failure to notify next of kin following violent assault and hospitalization; failure to ensure inmate safety; tolerance of prolonged SHU confinement under unsafe conditions; denial of transparency; supervisory failure.
Medical Services Department — USP Pollock (Staff Names Withheld Pending Disclosure)
Alleged conduct: Failure to follow established protocols for orbital and facial fractures; denial and delay of medical care; failure to explain treatment; refusal to provide medical records; inadequate pain management; deliberate indifference to worsening neurological and visual symptoms.
Special Housing Unit Staff — USP Pollock
Alleged conduct: Maintaining inhumane SHU conditions including lack of running water, extreme temperatures, contaminated food, and deprivation of basic hygiene; failure to ensure access to medical care.
KEY ALLEGATIONS & VIOLATIONS
| # | Allegation | Policy / Law Implicated | Impact |
| 1 | Failure to notify next of kin following violent assault and hospitalization | 18 U.S.C. § 4042 | Family left uninformed; safety risk |
| 2 | Denial and delay of medical care following traumatic injury | PS 6031.04; PS 6000.05; Eighth Amendment | Risk of permanent injury |
| 3 | Improper SHU confinement under inhumane conditions | 18 U.S.C. § 4042; Eighth Amendment | Physical and psychological harm |
| 4 | Failure to follow fracture and eye-injury protocols | Medical standards of care | Vision loss risk |
| 5 | Contaminated and inadequate food service | PS 4700.07 | Health risk |
| 6 | Lack of access to clean water and sanitation | Eighth Amendment | Disease risk |
| 7 | Obstruction of medical records and information | Due Process | Inability to advocate or treat |
| 8 | Deliberate indifference to escalating neurological symptoms | Eighth Amendment | Permanent disability |
| 9 | Failure of institutional transparency and accountability | 18 U.S.C. § 4042(a)(2) | Systemic liability |
EXPANDED ALLEGATION DETAIL
Allegation 1: Failure to Notify Next of Kin Following Violent Assault
Based on corroborated reporting reviewed by Loved Ones Coalition, an incarcerated individual at USP Pollock was violently assaulted on December 6, 2025, sustaining severe facial trauma and requiring outside hospitalization. Despite the seriousness of the injuries, the individual’s lawful spouse and designated emergency contact was not notified by the institution.
Family members were forced to rely on secondhand information from other incarcerated individuals to confirm the individual’s survival, condition, and location. This failure represents a serious breach of duty of care and family notification protocols.
Allegation 2: Denial and Delay of Medical Care Following Traumatic Injury
Based on corroborated reporting reviewed by Loved Ones Coalition, following the assault, the individual sustained a fractured face and orbital injury, including a broken eye socket. Despite these injuries, medical follow-up was delayed, inconsistent, and inadequate.
Reports indicate the individual declined certain medical encounters due to being confined in SHU conditions where care was not reliably provided. Even when medical contact occurred, the individual was not informed of treatment purpose, medication rationale, or long-term prognosis.
Allegation 3: Inhumane SHU Conditions
Based on corroborated reporting reviewed by Loved Ones Coalition, SHU conditions at USP Pollock include:
- Lack of running water, requiring individuals to drink water from their hands
- Extreme cold temperatures requiring use of showers to warm cells
- Food served cold, spoiled, or contaminated (including foreign objects)
- Lack of clean clothing exchange
- Unsanitary conditions incompatible with medical recovery
These conditions are incompatible with recovery from traumatic injury and pose serious health risks.
Allegation 4: Failure to Follow Eye-Injury and Fracture Protocols
Based on corroborated reporting reviewed by Loved Ones Coalition, medical staff reportedly acknowledged internally that proper protocols for orbital fracture injuries were not being followed but refused to disclose the correct protocol or provide timely corrective care.
Subsequent medical reporting indicated the injury may result in permanent blindness in the affected eye. Despite this, care remained delayed, fragmented, and inadequately explained.
Allegation 5: Obstruction of Medical Records and Information
Based on corroborated reporting reviewed by Loved Ones Coalition, requests for medical records were denied or delayed, with individuals being told records would not be available for six months or more. This obstruction prevents meaningful advocacy, second opinions, or external review.
Allegation 6: Escalating Neurological and Visual Symptoms Ignored
Based on corroborated reporting reviewed by Loved Ones Coalition, the individual experiences worsening symptoms including:
- Severe light sensitivity
- Persistent headaches
- Facial numbness
- Blurred vision
- Psychological deterioration due to isolation
Despite these symptoms, staff repeatedly minimized concerns and attributed symptoms to “healing” without adequate diagnostic support.
CONDITIONS & DIRECT TESTIMONY
“They have no running water. He’s drinking water out of his hands.”
— Reporting source
“The SHU is freezing cold. They turn the shower on to heat the cell.”
— Reporting source
“He was hit in the eye with a padlock. His eye socket is broken in multiple places.”
— Reporting source
“They told him he may go blind in his left eye.”
— Reporting source
PATTERN OR PRACTICE FINDINGS
- Violent incidents followed by isolation rather than protection
- Medical care conditioned on remaining in inhumane SHU confinement
- Chronic failure to notify families after serious injury
- Medical transparency systematically obstructed
- SHU conditions incompatible with medical recovery
- Institutional minimization of life-altering injuries
These findings establish systemic misconduct and deliberate indifference, not isolated error.
OVERSIGHT DEMANDS — USP POLLOCK
Loved Ones Coalition formally demands:
- Immediate referral of USP Pollock to the DOJ Office of Inspector General
- Preservation of all records related to the December 6, 2025 assault
- Preservation of all medical, SHU, and transfer records
- Independent medical review of eye and facial fracture treatment
- Immediate review of SHU conditions and food service
- Disclosure of family notification failures
- Congressional notification and inquiry
- Written assurances of non-retaliation
Failure to act will be documented as institutional complicity.
SOURCE PROTECTION STATEMENT
Loved Ones Coalition does not Distribution does not disclose the identity or classification of reporting sources. Information contained in this report is derived from corroborated documentation, testimony, and records reviewed by the organization. This intentional source protection is necessary due to documented patterns of retaliation within the Federal Bureau of Prisons. Staff names are included deliberately and in full when identified, as public servants acting under color of federal authority.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
SOUTH CENTRAL REGION
FCC Yazoo City (Low) — Mississippi
1. SUMMARY OF ALLEGATIONS
The Loved Ones Coalition has received direct, named allegations involving staff misconduct, physical abuse, verbal threats, retaliation, and interference with legal counsel at FCC Yazoo City Low.
According to reports provided to LOC, an incarcerated individual has been physically assaulted, verbally threatened, and intimidated by three named staff members, resulting in visible injuries, significant weight loss, and extreme fear for personal safety.
The reporting party states that abuse escalated to the point that they felt compelled to personally visit the facility to assess the individual’s condition, where the individual was observed beaten, physically marked, and severely weakened.
There is an expressed fear that continued exposure to these staff members poses a credible risk of serious bodily harm or death.
2. NAMED STAFF – KEY ALLEGATIONS & VIOLATIONS TABLE
| Staff Name | Alleged Conduct |
| Mr. Anderson | Physical assault, verbal threats, intimidation |
| Mr. Enderson | Physical abuse, participation in threats and retaliation |
| Ms. Ellis | Verbal abuse, intimidation, interference with communication |
3. DETAILED ALLEGATIONS
According to information provided to Loved Ones Coalition:
- The incarcerated individual is housed at FCC Yazoo City Low
- Mr. Anderson, Mr. Enderson, and Ms. Ellis are identified as the primary staff responsible
- The individual has allegedly been:
- Beaten
- Verbally threatened
- Intimidated
- When the individual’s attorney attempts to communicate, staff allegedly:
- Place the phone on speaker
- Remain present during the call
- Prevent the individual from speaking freely
- The reporting party states they went to the camp personally due to fear for the individual’s life
- During the visit, the individual was observed:
- Visibly bruised
- Extremely thin
- Marked from physical abuse
4. DIRECT TESTIMONY (SOURCE CONFIRMED, IDENTITY PROTECTED)
“It is Yazoo City Low. There are three people — Mr. Anderson, Mr. Enderson, and Ms. Ellis.”
“They threaten him verbally and with blows.”
“When the lawyer calls, they put the phone on speaker so they can hear everything.”
“I had to go see him myself. I saw him beaten, very thin. I am afraid they are going to kill him.”
5. PATTERN & ESCALATION CONCERNS
Loved Ones Coalition identifies critical escalation indicators, including:
- Named staff accused of coordinated misconduct
- Physical injuries witnessed by an outside party
- Interference with attorney–client privilege
- Fear of lethal retaliation
- Direct identification of multiple staff acting together
- Reported intimidation escalating over time
These indicators meet the threshold for immediate external oversight.
6. OVERSIGHT DEMANDS
Loved Ones Coalition formally demands:
- Immediate removal of Mr. Anderson, Mr. Enderson, and Ms. Ellis from any direct contact with the impacted individual
- Preservation of all:
- Surveillance footage
- Attorney call recordings/logs
- Staff duty rosters
- Incident reports
- Independent investigation into allegations of:
- Physical abuse
- Threats
- Retaliation
- Legal interference
- Immediate safety assessment and protective measures for the incarcerated individual
- Written confirmation that no retaliation will occur against the individual or reporting parties
- External oversight review if internal controls cannot ensure safety
7. SOURCE & DISCLOSURE STATEMENT
This report is based on direct information provided to Loved Ones Coalition, including firsthand observation by a reporting party.
Source identity is withheld to prevent retaliation.
LOC does not disclose whether information originated from incarcerated individuals, visitors, or family members.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
SOUTH CENTRAL REGION
FCI Texarkana — Texas
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, FCI Texarkana is experiencing systemic failures in environmental safety, sanitation, and First Step Act (FSA) sentence computation, resulting in unsafe living conditions and deprivation of statutory benefits. Documented reports describe widespread mold contamination, staffing failures within case management, and ongoing miscalculation and obstruction of FSA credits, with retaliatory behavior reported when incarcerated individuals seek clarification or attempt to use administrative remedies.
These failures reflect patterned neglect, not isolated incidents, and raise serious concerns regarding compliance with federal law and Bureau of Prisons policy.


KEY ALLEGATIONS & VIOLATION TABLE
| Allegation Category | Description | Implicated Policy / Law |
| Environmental Health & Safety | Extensive visible mold contamination in shower and housing areas, including ceilings and ventilation surfaces | PS 1600.11 (National Occupational Safety & Environmental Health); 18 U.S.C. § 4042 |
| Sanitation Failures | Failure to remediate known mold conditions despite prolonged exposure | PS 4200.12 (Facilities Operations) |
| FSA Credit Miscalculation | Improper calculation and failure to apply earned First Step Act credits | PS 3710.01; 18 U.S.C. § 3632 |
| Case Management Neglect | Excessive caseloads resulting in inaccurate release dates and lack of assistance | PS 5322.13 (Unit Management) |
| Obstruction of Administrative Remedies | Hostile responses and refusal to assist when inmates inquire about sentence computation; BP remedies delayed | PS 1330.18 (Administrative Remedy Program) |
DETAILED ALLEGATIONS
1. Environmental & Mold Exposure Hazards
According to multiple reporting sources, incarcerated individuals at FCI Texarkana are housed in units with visible mold growth on ceilings, structural seams, and ventilation-adjacent surfaces, particularly in shower and hygiene areas. Photographic documentation reviewed by LOC shows active mold colonies, staining, and moisture damage consistent with prolonged neglect.
These conditions pose documented respiratory and dermatological health risks, particularly in congregate living environments, and indicate a failure to conduct adequate inspection, remediation, or preventive maintenance.
2. Failure to Properly Calculate and Apply FSA Credits
Based on verified documentation and testimony, individuals at FCI Texarkana report incorrect First Step Act time credit calculations, delayed application of earned credits, and inaccurate projected release or placement dates.
Affected individuals report that inquiries regarding sentence computation are met with hostility rather than assistance, leaving incarcerated people without clarity on their lawful release timelines.
3. Case Management Breakdown and Improper Caseload Allocation
Through documented reports reviewed by LOC, the assigned case manager is responsible for an excessive caseload of approximately 250 incarcerated individuals, far exceeding reasonable management standards. This has resulted in missed updates, incorrect dates, and failure to process FSA-related actions.
When individuals seek clarification or correction, reports indicate dismissive conduct and refusal to provide meaningful assistance.
4. Obstruction and Retaliatory Conduct Related to Remedies
According to sources with direct knowledge of facility operations, individuals who question sentence computation errors or request clarification are met with dismissive and hostile responses, discouraging use of administrative remedies. At least one individual reports preparing to escalate to a BP-10 due to lack of institutional response.
This conduct undermines access to remedies and raises concerns of retaliation through obstruction, in violation of BOP policy.
NAMED STAFF IMPLICATED (ACCOUNTABILITY INDEX)
All named staff are public servants acting under color of federal authority.
- Ms. Robinson — Case Manager
Alleged Conduct:
- Failure to properly calculate and apply First Step Act credits
- Inaccurate release and placement dates
- Hostile and dismissive conduct when questioned
- Failure to provide assistance consistent with case management duties
Referenced In: Allegations 2, 3, and 4
PATTERN OR PRACTICE FINDINGS
- Repeated reports of FSA credit miscalculation tied to the same case management function
- Chronic environmental hazards with no evidence of remediation
- Staff workload mismanagement resulting in systemic harm
- Consistent discouragement of administrative remedy use
- Failures persist despite prior notice and reporting
These findings establish systemic liability rather than isolated misconduct.
OVERSIGHT DEMANDS
Loved Ones Coalition formally demands:
- Immediate environmental inspection and independent mold remediation assessment
- Preservation of all facility maintenance, inspection, and sanitation records
- Full audit of First Step Act credit calculations for affected individuals
- Immediate review of case management staffing and workload allocation
- Referral of documented failures to the DOJ Office of Inspector General
- Protection from retaliation for individuals cooperating with oversight
SOURCE PROTECTION STATEMENT
Loved Ones Coalition does not disclose the identity or classification of reporting sources. Information contained in this report is derived from corroborated documentation, testimony, and records reviewed by the organization. This intentional source protection is necessary due to documented patterns of retaliation within the Federal Bureau of Prisons. Staff names are included deliberately and in full, as public servants acting under color of federal authority.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
NORTH CENTRAL REGION
USP Terre Haute — Indiana
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, conditions at USP Terre Haute reflect severe sanitation failures, pest infestation, and prolonged restrictive housing practices, creating unsafe and degrading living conditions. Documented reports describe roach and rodent infestations throughout housing areas, chronic lockdowns, and conditions so extreme that individuals with prior federal incarceration experience report them as unprecedented.
These conditions raise serious concerns regarding compliance with federal statutory duties to ensure safe, humane confinement.
KEY ALLEGATIONS & VIOLATION TABLE
| Allegation Category | Description | Implicated Policy / Law |
| Pest Infestation | Widespread roach and mouse infestations reported in housing areas | PS 1600.11 (Environmental Health & Safety); 18 U.S.C. § 4042 |
| Sanitation Failures | Inadequate pest control and environmental maintenance | PS 4200.12 (Facilities Operations) |
| Prolonged Lockdowns | Frequent and extended lockdowns restricting movement and access | PS 5500.15 (Correctional Services Procedures) |
| Unsafe Living Conditions | Conditions described as extreme even by individuals with prior federal incarceration experience | Eighth Amendment standards; 18 U.S.C. § 4042 |
DETAILED ALLEGATIONS
1. Severe Pest Infestation
According to multiple reporting sources, housing units at USP Terre Haute are infested with roaches and mice, with pests observed in living areas on a routine basis. Reports indicate that infestation is ongoing, not episodic, and that adequate pest mitigation measures are either ineffective or not being implemented.
Such conditions present clear health risks, including contamination of food, bedding, and personal property, and indicate systemic failures in sanitation and facility maintenance.
2. Chronic Lockdowns and Restrictive Conditions
Based on verified documentation and testimony, individuals at USP Terre Haute report being placed on frequent and prolonged lockdowns, with limited explanation or transparency regarding duration or justification. These lockdowns compound already hazardous living conditions by restricting access to showers, recreation, and normal movement.
The frequency and severity of these restrictions exceed what is reasonably necessary for institutional safety and raise concerns regarding improper use of restrictive housing practices.
3. Conditions Exceeding Prior Federal Confinement Experiences
Through documented reports reviewed by LOC, at least one individual with previous federal incarceration history stated that conditions at USP Terre Haute are worse than any federal facility previously experienced. This comparative assessment underscores the severity of the reported conditions and suggests a marked deviation from baseline federal standards.
PATTERN OR PRACTICE FINDINGS
- Persistent pest infestations without effective remediation
- Chronic environmental neglect within housing units
- Repeated lockdowns used as a default operational condition
- Conditions deteriorating beyond accepted federal confinement norms
These findings demonstrate systemic environmental and operational failure, not isolated maintenance issues.
OVERSIGHT DEMANDS
Loved Ones Coalition formally demands:
- Immediate independent environmental health and pest control inspection
- Preservation of all sanitation, maintenance, and pest control records
- Review of lockdown frequency, duration, and authorization practices
- Corrective action to restore humane living conditions
- Referral of documented conditions to the DOJ Office of Inspector General
- Protection from retaliation for individuals providing information
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
NORTH CENTRAL REGION
USP Leavenworth
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, USP Leavenworth is operating under near-constant lockdown conditions resulting in systemic deprivation of food access, commissary access, and basic necessities. Documented reports indicate a recurring pattern in which lockdowns are deliberately imposed on scheduled commissary days, followed by denial of make-up access, effectively extending deprivation for weeks at a time.
These conditions raise serious concerns regarding compliance with federal obligations to provide adequate nutrition and access to commissary services essential for daily living.
KEY ALLEGATIONS & VIOLATION TABLE
| Allegation Category | Description | Implicated Policy / Law |
| Food Deprivation | Inadequate meal access during extended lockdowns | PS 4700.07 (Food Service Manual); 18 U.S.C. § 4042 |
| Commissary Denial | Lockdowns imposed on commissary days with no make-up access | PS 4500.12 (Trust Fund/Commissary Operations) |
| Prolonged Lockdowns | Repeated and near-continuous lockdown status | PS 5500.15 (Correctional Services Procedures) |
| Deprivation of Basic Needs | Inmates unable to supplement inadequate meals due to commissary denial | Eighth Amendment standards |
DETAILED ALLEGATIONS
1. Chronic Lockdowns Resulting in Food Deprivation
According to multiple reporting sources, USP Leavenworth has been on almost constant lockdown for an extended period. During these lockdowns, individuals report insufficient food portions, with meals failing to meet basic caloric needs.
The lack of adequate nutrition is compounded by the inability to access commissary items that would otherwise supplement meals, resulting in sustained deprivation.
2. Manipulation of Commissary Access
Based on verified documentation and testimony, individuals report a recurring pattern in which lockdowns are initiated on scheduled commissary days. When lockdowns coincide with commissary schedules, access is canceled outright.
Rather than providing make-up commissary access once lockdowns are lifted, individuals are reportedly told they must wait until the following scheduled commissary day—only for lockdowns to be reinstated again. This cycle has resulted in weeks-long denial of commissary access.
3. Systemic Deprivation of Basic Necessities
Through documented reports reviewed by LOC, individuals report that the combined impact of inadequate meals and denied commissary access has left them without essential items, including food, hygiene products, and basic personal supplies.
This practice effectively converts lockdown status into a mechanism of prolonged deprivation rather than a temporary security measure.
PATTERN OR PRACTICE FINDINGS
- Lockdowns repeatedly aligned with commissary schedules
- No make-up commissary access following lockdown cancellations
- Inadequate food provision during prolonged lockdowns
- Deprivation of basic necessities extending for weeks at a time
These findings establish a pattern of systemic deprivation, not isolated operational disruptions.
OVERSIGHT DEMANDS
Loved Ones Coalition formally demands:
- Immediate review of lockdown authorization practices and scheduling
- Preservation of all commissary schedules, cancellation logs, and lockdown records
- Independent audit of food service adequacy during lockdown periods
- Corrective action to ensure make-up commissary access following lockdowns
- Referral of documented conditions to the DOJ Office of Inspector General
- Protection from retaliation for individuals providing information
SOURCE PROTECTION STATEMENT
Loved Ones Coalition does not disclose the identity or classification of reporting sources. Information contained in this report is derived from corroborated documentation, testimony, and records reviewed by the organization. This intentional source protection is necessary due to documented patterns of retaliation within the Federal Bureau of Prisons. Staff names are included deliberately and in full, as public servants acting under color of federal authority.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
NORTH CENTRAL REGION
FCI Thomson — Illinois
Summary of Allegations
Multiple incarcerated individuals and family members report systemic medical neglect, manipulation of Care Level classifications, prolonged communication blackouts, retaliatory lockdown practices, and denial of prerelease opportunities at FCI Thomson. Evidence indicates a pattern of administrative misconduct designed to conceal the true number of aging and medically vulnerable prisoners, while simultaneously restricting access to treatment, diagnostic services, and outside oversight.
Reports further document extended isolation without notice, refusal to provide timely welfare confirmations to families, and staff behavior inconsistent with Bureau of Prisons policy governing humane treatment, medical care, and transparency.
Key Allegations & Violations Table
| Category | Allegation | Details / Evidence | Potential Policy Violations |
| Medical Neglect | Care Level manipulation | Care Level 3 AICs approved for medical transfer were denied without explanation; staff later stated “lack of beds” | 18 U.S.C. § 4042(a)(2); BOP Clinical Care Levels Policy |
| Medical Fraud / Misclassification | Artificial downgrading of care levels | A physician waved a document referencing a “new algorithm” used to downgrade Care 3 prisoners, creating false appearance of improved health | False Records / Deliberate Indifference |
| Diagnostic Delays | X-ray facility unusable | State-of-the-art X-ray unit has no technician; prisoners sent offsite quarterly, causing up to 1-year delays | 28 C.F.R. § 549.10 |
| Surgical Delays | Untreated hernias | AICs walking with hernias 5–30 cm, discoloration (blue/purple), poor vascularization; some waiting 5+ years | Eighth Amendment |
| Communication Blackouts | No contact for 15+ days | Families unable to confirm whether loved ones were alive; staff responses dismissive | PS 5265.14 |
| Retaliatory Lockdowns | Mass punishment | Entire dorms locked down for actions in unrelated housing units | Due Process Violations |
| Prerelease Denials | First Step Act noncompliance | Denial of halfway house, First Step, and Second Chance Act placements | FSA / SCA Violations |
| Financial Exploitation | Illegal notary fees | Reports of $2,000 charges for notary services via staff contacts | Fraud / Abuse of Authority |
| Discrimination | Job access inequity | Black incarcerated individuals report denial of jobs and unequal treatment | Civil Rights Violations |
Pattern & Risk Assessment
- Medical data manipulation suggests intentional underreporting of high-care prisoners
- Delayed diagnostics and surgeries place incarcerated individuals at serious risk of permanent injury or death
- Communication suppression creates life-or-death uncertainty for families
- Retaliation culture deters grievances and whistleblowing
- Cost-inefficient outsourcing contradicts fiscal responsibility claims
This pattern reflects systemic institutional failure, not isolated misconduct.
Oversight Demands
- Immediate external audit of Care Level classifications and medical transfer denials
- Independent medical review of all untreated hernia cases and delayed surgeries
- Staffing emergency hire for diagnostic imaging personnel
- Preservation of all records related to Care Level “algorithm” changes
- DOJ OIG investigation into financial exploitation and notary fee allegations
- Family communication protocol enforcement with welfare verification timelines
- Retaliation monitoring with protections for reporting AICs
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
WESTERN REGION
USP Victorville — California
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, USP Victorville has engaged in a pattern of excessive force, misuse of “stop resisting” commands to justify assaults, prolonged lockdowns without required hygiene access, sanitation failures, and staff indifference to basic living conditions.
Reported incidents span December 2025 through January 2026 and include a documented physical assault by a named correctional officer, followed by extended lockdown conditions in which incarcerated individuals were denied showers, forced to live among accumulated trash, and provided conflicting or false explanations by staff regarding operational responsibilities.
These incidents reflect failures in use-of-force compliance, sanitation standards, and lockdown management protocols.
KEY ALLEGATIONS & POLICY VIOLATIONS TABLE
| Allegation | Date | Location | Staff Implicated | Policy / Standard Implicated |
| Physical assault of inmate near cell door followed by false “stop resisting” commands | Nov 2025 (pre-Thanksgiving) | USP Victorville | Officer Robles | 18 U.S.C. § 4042; BOP Use of Force Policy |
| Misuse of verbal commands to justify force after assault | Nov 2025 | USP Victorville | Officer Robles | BOP Use of Force Reporting Standards |
| Lockdown imposed following alleged escape attempt | Dec 25, 2025 | USP Victorville | Facility Staff | BOP Lockdown & Emergency Operations Policy |
| Denial of all showers during week-long lockdown | Dec 25–31, 2025 | USP Victorville | Facility Staff | BOP Hygiene & Sanitation Standards |
| Accumulation of trash for multiple days without removal | Dec 25–28, 2025 | USP Victorville | Facility Staff | BOP Environmental Health & Sanitation Policy |
| Staff refusal to address sanitation, citing “next shift” | Dec 2025 | USP Victorville | Facility Staff | Duty of Care / Facility Operations |
DETAILED INCIDENT NARRATIVE
Use of Force Incident — Officer Robles
According to multiple reporting sources, a few days prior to Thanksgiving 2025, an incarcerated individual was late exiting the computer area before lockdown and ran upstairs to reach his assigned cell. The individual had reached his cell door when Officer Robles initiated a physical assault without provocation.
Witnesses report that once the assault began, Officer Robles repeatedly shouted “Stop resisting!” despite the inmate being at his cell door. The timing and repetition of these commands appeared to occur after the physical contact had already begun and were perceived as an attempt to justify the use of force once witnesses were present.
No resistance was observed prior to the assault. The verbal commands were issued only after the officer initiated contact.
Lockdown Conditions — December 25, 2025
Based on verified documentation and testimony, USP Victorville entered lockdown status on Christmas Eve 2025 due to flood warnings. On Christmas Day, doors were initially opened at normal times but were locked down again immediately after breakfast.
Staff advised incarcerated individuals that the lockdown resulted from an attempted escape. Reports indicate the individual involved removed his uniform, wore street clothing, and passed through two gates before being stopped.
The lockdown lasted approximately one week.
Hygiene & Sanitation Failures During Lockdown
Through documented reports reviewed by LOC, the following conditions occurred during the lockdown:
- Zero showers provided for the entire duration, despite BOP policy requiring three showers per week
- Styrofoam food trays and trash accumulated inside housing units for approximately three days
- Trash was not collected despite repeated requests
- Officers responded that they were “not told to do it” or that “the next shift would handle it”
Trash remained in living areas, creating unsanitary conditions and exacerbating health risks.
PATTERN OR PRACTICE FINDINGS
The incidents at USP Victorville demonstrate a pattern of operational failure, not isolated events:
- Use-of-force incidents followed by verbal commands to retroactively justify officer actions
- Lockdowns imposed without compliance with hygiene and sanitation requirements
- Repeated deflection of responsibility by staff (“next shift” explanations)
- Lack of accountability during emergency operations
These conditions reflect systemic breakdowns in supervision, training, and enforcement of BOP policy.
NAMED STAFF IMPLICATED (ACCOUNTABILITY INDEX)
- Officer Robles — Correctional Officer
Alleged conduct: Initiated an unprovoked physical assault and used verbal “stop resisting” commands after force was applied
Referenced in: Allegation 1
OVERSIGHT DEMANDS
Loved Ones Coalition issues the following demands, not requests:
- Immediate removal of Officer Robles from direct inmate contact pending investigation
- Preservation of all use-of-force reports, body camera footage (if applicable), and incident logs related to the November 2025 assault
- Referral of this matter to the DOJ Office of Inspector General
- Independent review of lockdown operations and hygiene compliance from December 25–31, 2025
- Congressional notification regarding sanitation and lockdown policy violations at USP Victorville
SOURCE PROTECTION STATEMENT
Loved Ones Coalition does not disclose the identity or classification of reporting sources. Information contained in this report is derived from corroborated documentation, testimony, and records reviewed by the organization. This intentional source protection is necessary due to documented patterns of retaliation within the Federal Bureau of Prisons. Staff names are included deliberately and in full, as public servants acting under color of federal authority.
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT
WESTERN REGION
FCI Terminal Island — California
SUMMARY OF ALLEGATIONS
Based on corroborated reporting reviewed by Loved Ones Coalition, FCI Terminal Island is engaging in opaque and unsafe operational practices amid an anticipated facility closure, resulting in severe anxiety among incarcerated individuals and their families, unannounced visitation denials, inconsistent and misleading lockdown status reporting, prolonged communication blackouts, and failure to safeguard medically vulnerable populations during infrastructure failures.
In addition to ongoing non-transparency surrounding visitation and potential population movement, new reporting confirms a significant electrical outage affecting large portions of the facility, resulting in loss of phone and email communications, cancellation of visits, and disruption of medical care. Individuals with chronic medical conditions, including diabetes, were reportedly left without access to necessary treatment or monitoring during the outage.
Families report traveling long distances only to be turned away without explanation. Incarcerated individuals report phones and email systems being completely down, staff refusing to clarify whether the facility was on lockdown, and a lack of emergency communication or medical contingency planning. These conditions raise serious concerns regarding due process, humane treatment, medical neglect, emergency preparedness, and administrative transparency.
KEY ALLEGATIONS & VIOLATIONS TABLE
| Allegation Category | Description of Conduct | Policy / Legal Implications |
| Unannounced Visitation Cancellations | Families arrived for scheduled visits and were denied entry without notice or explanation | PS 5267.09 – Visiting Regulations |
| Failure to Report Lockdown Status | Lockdowns or movement restrictions not reflected on BOP public systems | PS 5500.14 – Correctional Services Procedures |
| Communication Blackouts | Phones and email systems down for extended periods | PS 5264.08 – Inmate Telephone Regulations |
| Electrical Infrastructure Failure | Facility-wide or partial power outage disrupting operations | 18 U.S.C. § 4042(a)(2) |
| Medical Care Disruption | Individuals with chronic conditions (including diabetes) lacked access to care during outage | PS 6031.04; Eighth Amendment |
| Lack of Administrative Transparency | Staff instructed families to “call tomorrow” without clarifying status | 18 U.S.C. § 4042(a)(2) |
| Psychological Harm | Heightened anxiety due to uncertainty, outages, and lack of information | Eighth Amendment – Conditions of Confinement |
DETAILED FINDINGS
1. Visitation Interference and Public Misinformation
According to multiple reporting sources, visits were cancelled or denied without advance notice, despite no public indication of lockdown or emergency conditions on official Bureau of Prisons platforms. Families who traveled to the facility were turned away without explanation, written notice, or rescheduling guidance.
This conduct reflects failure to comply with visitation notice requirements and compounds family hardship.
2. Unreported Lockdowns, Power Failure, and Communication Collapse
Reporting received by Loved Ones Coalition confirms that large portions of FCI Terminal Island experienced a power outage, resulting in:
- Phone systems being completely down
- Email systems unavailable
- No visitation permitted
- No clear public or internal communication regarding facility status
Despite these conditions, staff reportedly denied that the facility was on lockdown and provided inconsistent explanations to families and incarcerated individuals. This discrepancy strongly suggests administrative concealment or mismanagement of emergency conditions.
3. Medical Risk During Electrical Outage
Critically, reporting indicates that incarcerated individuals with medical conditions were adversely impacted during the power outage, including individuals with diabetes who were reportedly unable to access necessary care, monitoring, or accommodations.
The absence of contingency planning, emergency medical communication, or documented safeguards during an electrical failure raises serious concerns regarding medical neglect and deliberate indifference, particularly given the known vulnerability of chronically ill populations in custody.
4. Facility Closure Anxiety and Due Process Failures
The anticipated closure of FCI Terminal Island has already generated widespread fear and uncertainty. The addition of unannounced outages, unexplained visitation denials, and communication blackouts has intensified distress among incarcerated individuals and families.
No formal notice, timeline, or explanation regarding transfers, housing changes, or visitation impacts has been provided. Families are left to rely on rumors, sporadic calls, or secondhand information, rather than lawful notice from the institution.
PATTERN OR PRACTICE FINDINGS
This conduct reflects a broader pattern of institutional non-transparency and operational failure, including:
- Failure to update public-facing systems during emergencies
- Withholding critical operational information from families
- Communication shutdowns without contingency planning
- Lack of medical safeguards during infrastructure failures
- Use of “call back tomorrow” in place of lawful notice
- Allowing uncertainty and medical risk to persist during major institutional changes
These practices expose the Bureau of Prisons to systemic liability, not isolated administrative error.
OVERSIGHT DEMANDS
Loved Ones Coalition formally demands:
- Immediate disclosure of the scope, duration, and cause of the electrical outage
- Written explanation for all visitation denials and communication outages during the reported period
- Preservation of all outage logs, maintenance records, call logs, email system records, and medical incident reports
- Independent review of medical care continuity during the power failure
- Disclosure of emergency preparedness and contingency protocols
- Congressional notification regarding facility closure procedures and infrastructure failures
- DOJ Office of Inspector General review of transparency, medical risk, and emergency response failures
LOVED ONES COALITION
FEDERAL OVERSIGHT REPORT